
Wound Healing
Discover how Melior’s unique phenotypic screening platforms can uncover the untapped value of your candidate therapeutic
Impaired wound healing is responsible for significant morbidity and mortality worldwide. The process of wound healing is complex, involving a number of biological pathways that become activated after tissue injury. This process can become impaired under a number of conditions, such as in diabetic subjects, leading to complications such as higher susceptibility to infection and / or amputation. Agents that promote epithelialization, cellular proliferation or angiogenesis may improve the wound healing process.
Rodents represent an ideal preclinical model, as they are economical and amenable to genetic manipulation, which allows for mechanistic investigation. While requiring consistency and care, this model does not involve complicated surgical techniques and allows for the relatively robust testing of promising agents that may, for example, promote angiogenesis or inhibit inflammation.
The most common and simple way of studying wound healing in rodents involves creating a standardized wound with a skin biopsy punch. The model can be setup in way such that each animal serves as its own control by applying two wounds to either side of the animal—one treated and one untreated or vehicle-treated. Evaluation of wound diameter over time as well as time to wound closure is a simple, cost-effective way of measuring the healing process. Melior also routinely includes histological evaluations in our wound healing studies.
The study illustrated below shows the effect of a diabetic condition on wound closure rate in diabetic rats (Zucker diabetic fatty fa/fa (ZDF)).
Ready to get started or looking for a custom model?
Contact us today for more information about our bespoke research models and to discuss how we can help you answer your unique research questions.
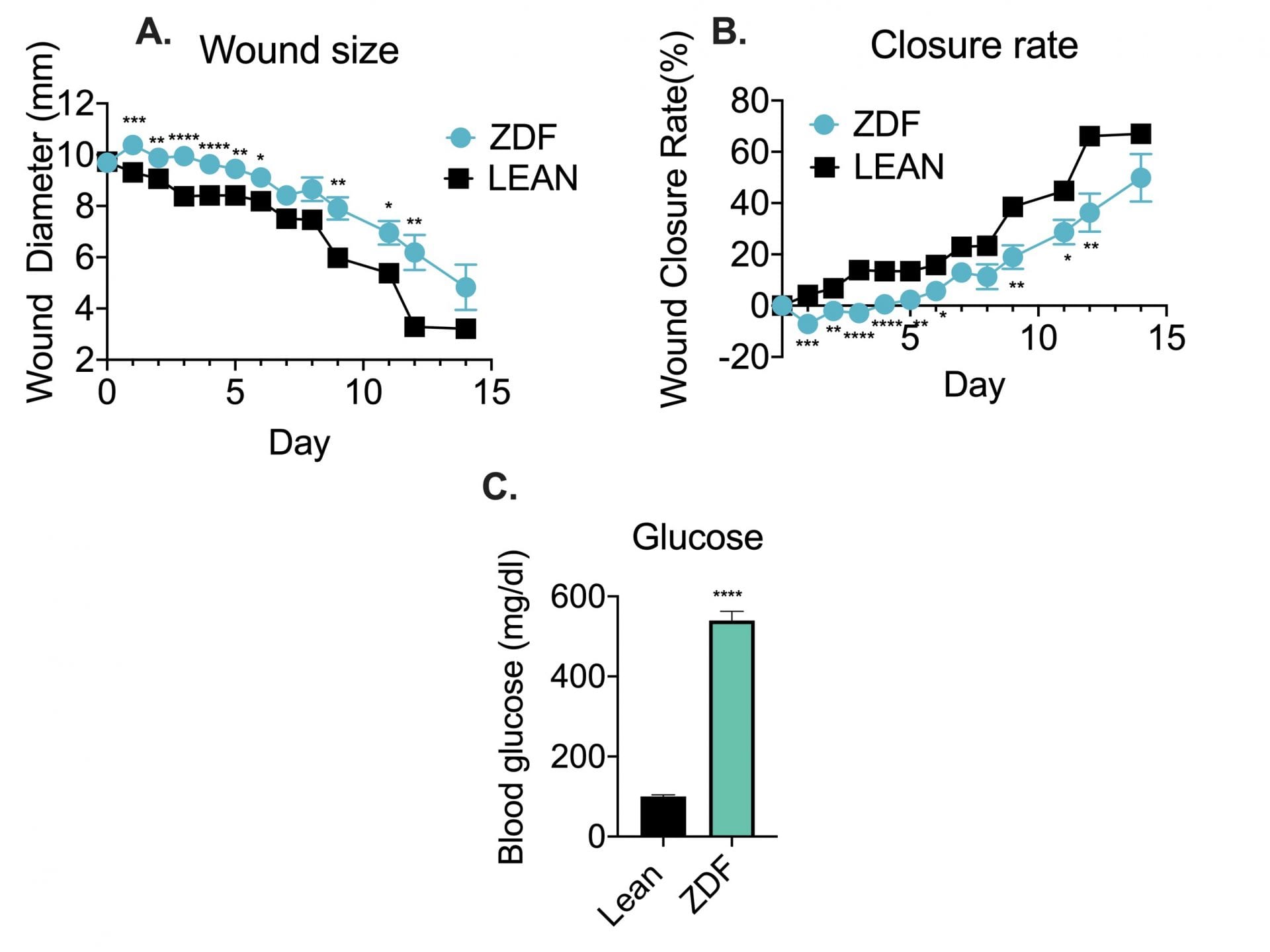
Male ZDF rats were anesthetized, shaved and prepped. 10-mm wounds (bilateral) were generated via a punch biopsy on the dorsal skin towards the scapular region. Following the wound excision, wounds were covered with Tegaderm™ (3M) dressing. Wound dressing was changed on the Days of wound measurement, i.e. Day 0, 1, 2, 3,4,5,6,7,8, 9,11, 12 and 14. Animals were individually housed to protect the wound. A. Wound sizes were measured with a digital caliper (mm). B. The wound closure rates were also calculated based on the wound size of pre-treatment (Day 1, prior to first injection). C. Blood glucose measurements were performed at baseline and once per week during the study. Figure C shows blood glucose at baseline. No significant difference of blood glucose was observed over the course of the study.
Data are mean ±SEM analyzed using a t-test. (N=12) * p< 0.05, **p<0.01, *** p<0.001, **** p< 0.0001.
This is a sub-chronic model evaluating effects of test articles (typically with multiple administrations). Group sizes of 8 to 10 are conventional. It works well in both rats and mice. It also works in specialty model such as diabetes models such a STZ-insulin-depleted rat model.
Frequently Asked Questions
We routinely use the excisional splinted full-thickness wound model on the dorsum of the mouse to prevent wound contraction and ensure healing is driven by re-epithelialization and granulation tissue formation. The primary efficacy endpoint is the quantification of the wound area over time, expressed as a percentage of the initial wound size, measured via digital photography and specialized image analysis software.
A typical study duration for monitoring full wound closure is between 10 to 14 days, with wound area measurements taken every 2-3 days.
Commonly used models include excisional (full-thickness punch biopsy), incisional, and burn wound models. For impaired healing research, diabetic wound models (db/db mice or ZDF rats) better mimic human healing — are also available.
Yes. Study designs can be customized across species(rat vs mice) and strain selection, wound size, treatment route and dosing schedule, and tissue collection time points. Both prophylactic and therapeutic paradigms can be accommodated, and serial wound photography with digital planimetry enables longitudinal tracking of wound closure.
Yes. Standard histological endpoints include H&E for re-epithelialization and inflammation, and Masson’s Trichrome or Sirius Red for collagen deposition. Molecular endpoints such as cytokine and growth factor profiling (e.g., TGF-β, VEGF), immunohistochemistry, and gene expression analysis can also be added for mechanistic evaluation.
Rodent wound healing models are well-validated for preclinical efficacy testing, with the diabetic wound model offering particularly strong clinical relevance. A key limitation is that rodents heal predominantly via wound contraction rather than re-epithelialization; the splinted wound model partially addresses this by better mimicking human skin healing.

Interested in running a Wound Healing study?
If you are interested in learning more about the Wound Healing Model, please contact us to start the conversation today!